
This advertorial is sponsored by Alio Medical
 Owing to the various risk factors and potential complications faced by kidney disease patients undergoing dialysis treatment, new technologies that enable these patients to be monitored remotely and continuously—and ultimately managed more effectively—are a critical necessity. David Whittaker (Suburban Hospital, Bethesda, USA), Qasim Butt (Metropolitan Methodist Hospital, San Antonio, USA), Anand Patel (Providence Little Company of Mary Medical Centers, Torrance, USA) and Carole Sykes (Clinical Strategy Group, San Francisco Bay Area, USA) highlight one such innovation, the SmartPatch device, and the broad array of problems it is seeking to tackle.
Owing to the various risk factors and potential complications faced by kidney disease patients undergoing dialysis treatment, new technologies that enable these patients to be monitored remotely and continuously—and ultimately managed more effectively—are a critical necessity. David Whittaker (Suburban Hospital, Bethesda, USA), Qasim Butt (Metropolitan Methodist Hospital, San Antonio, USA), Anand Patel (Providence Little Company of Mary Medical Centers, Torrance, USA) and Carole Sykes (Clinical Strategy Group, San Francisco Bay Area, USA) highlight one such innovation, the SmartPatch device, and the broad array of problems it is seeking to tackle.
The chronic kidney disease (CKD) patients’ complications include volume overload, hyperkalaemia, malignant hypertension, and worsening heart failure—many of which could potentially be preventable with improved disease monitoring. In 2017, there were almost 800 million people suffering from CKD worldwide, including 39 million in the USA alone. As per a recent systematic review published in The Lancet, it is estimated to become the fifth leading cause of death globally by 2040. The natural progression of CKD is complex and involves multiple organ systems. As a result, these patients commonly present to emergency rooms (ER) 8.5 times more frequently than the general population and the prevalence of these ER visits is highest in the seven days prior to beginning dialysis.
Of all the end-stage kidney disease (ESKD) patients seen in the ER, the mean number of visits per patient year in the first, second and third years of their disease was 2.89, 2.48, and 2.54 per year, respectively, according to a population-based study. And, in another study using Medicare data, more than 131,000 of at least 11 million total ER visits were for hyperkalaemia and fluid overload in the ESKD population.
ER visits for hyperkalaemia were common in a separate population-based analysis—particularly among patients on dialysis, where the condition accounted for almost one half (48.8%) of all potentially preventable visits. The analysis’ researchers showed a linear trend toward developing hyperkalaemia, with the highest rates among patients with non-dialysis-dependent Stage 5 CKD (22.9; 95% confidence interval [CI], 16.7 to 29.1 ER visits per 1,000 person years) and dialysis-dependent patients (22.4; 95% CI, 17.2 to 27.5 ER visits per 1,000 person years).
Several other groups have reported that early referral to nephrology results in better control of clinical parameters, for example blood pressure and serum levels of albumin, bicarbonate, calcium, cholesterol, haemoglobin, potassium, and phosphate. This suggests that making it easier to manage a patient’s health status could reduce the likelihood of emergent complications. In a more recent study, researchers showed that patients with early referrals and frequent physician visits were less likely to be hospitalised within one year of initiating dialysis, despite these patients being older and having higher Charlson comorbidity index scores.
The primary goals for nephrologists managing patients with ESKD are to lower mortality, extend renal function, and improve quality of life. In dialysed patients, preservation of residual renal function is associated with improved survival, lower morbidity and better quality of life.
A wearable, patient-centred management solution
In order to improve the nephrologist’s ability to optimise the overall outcomes of their ESKD population, Alio is in the process of developing an innovative device, called SmartPatch, to provide a continuous and comprehensive clinical management solution for both the nephrology team and the ESKD patient.
The Alio SmartPatch is a continuous, non-invasive, remote monitoring device that automatically sends clinically actionable data to a hub. It is worn directly over a patient’s arteriovenous fistula (AVF) or upper-extremity artery, and safely relays raw data via the hub to a cloud-based server where it is processed and analysed utilising proprietary algorithms. The server encrypts and stores the data without it being associated with a subject’s personal health information. This data collection process is invisible to the patient, who wears the SmartPatch and simply plugs the hub into a standard wall outlet in their home. There is no complex setup or configuration for the patient—the patch is worn while showering and sleeping, and typically changed at seven-day intervals.
 The data collected are always accessible to the clinical team via a Health Insurance Portability and Accountability Act (HIPAA)-compliant, web-based portal and notifications can be automatically sent to a designated provider if a clinically relevant abnormality is detected. And, in addition to recently receiving its first US Food and Drug Administration (FDA) 510(k) clearance for commercial use, Alio is undergoing multiple clinical evaluations. The parameters being evaluated for remote monitoring in these evaluations include haemoglobin, haematocrit, potassium, oxygenation saturation, heart rate, and 10–15 seconds of audio auscultation data from flow in the underlying AVF or arteriovenous graft (AVG).
The data collected are always accessible to the clinical team via a Health Insurance Portability and Accountability Act (HIPAA)-compliant, web-based portal and notifications can be automatically sent to a designated provider if a clinically relevant abnormality is detected. And, in addition to recently receiving its first US Food and Drug Administration (FDA) 510(k) clearance for commercial use, Alio is undergoing multiple clinical evaluations. The parameters being evaluated for remote monitoring in these evaluations include haemoglobin, haematocrit, potassium, oxygenation saturation, heart rate, and 10–15 seconds of audio auscultation data from flow in the underlying AVF or arteriovenous graft (AVG).
The data monitored by the SmartPatch are designed to enable improved management of the complex clinical aspects facing patients with CKD in an outpatient setting. This improvement in monitoring and outpatient management has the goal of also boosting patient outcomes, reducing adverse events, and reducing the burdens currently faced by emergency healthcare services.
Continuous remote monitoring also provides a new level of comfort for a patient who will, for the first time, know that their critical data can be quickly, safely and remotely accessed by their healthcare team. The advantage of this degree of close monitoring is that it provides the healthcare team with the management tools it needs to proactively intervene to optimise patient outcomes.
Hyperkalaemia and hypokalaemia
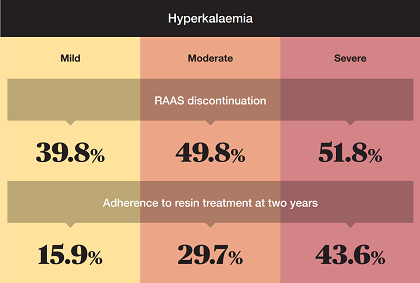
The kidneys play a crucial role in the regulation of potassium. Patients with CKD and ESKD are at risk of hyper/hypokalaemia (high/low potassium levels). Hypokalaemia is typically a consequence of diuretics, while hyperkalaemia is the most common imbalance due to loss of renal function—which becomes more prevalent as the disease progresses. Hyperkalaemia has been classified somewhat arbitrarily into mild (5.1–<6mmol/l), moderate (6–<7mmol/l) and severe (≥7mmol/l). Potassium levels >7mmol/l are of critical importance as the clinical symptoms can vary widely from nonspecific muscle weakness to paraesthesias and paralysis. These high levels may also be associated with cardiac arrhythmias and sudden cardiac death. Even though electrocardiogram (ECG) changes related to hyperkalaemia are diagnostically useful, they are notoriously poor at correlating with serum potassium levels; with studies indicating accuracy in only 40–50% of chronic hyperkalaemia patients.
A further complexity in the treatment of CKD is the recommended use of renin-angiotensin-aldosterone (RAAS) inhibitors to reduce disease progression and increase survival in patients with advanced CKD (Stage ≥3), diabetes, or chronic heart failure. These recommendations are supported by several professional societies, including the European Society of Cardiology, American College of Cardiology Foundation, American Heart Association and Heart Failure Society of America, as well as in the Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines. The sparing of residual renal function in these patients afforded by RAAS blockade is well-accepted, but RAAS blockade is also a known risk factor for hyperkalaemia in the CKD population. Continuous, non-invasive means of remotely monitoring potassium levels in the CKD population provide the data to alter current treatment paradigms.
The management of chronic hyperkalaemia is particularly challenging. The main objective of the emergency treatment of this indication is to prevent fatal arrhythmias—which is accomplished by facilitating the movement of extracellular potassium into the cell, stabilising myocardial cell membrane potentials pharmacologically, and quickly increasing potassium elimination from the body. This is typically accomplished using insulin to drive potassium into the cell, which serves as a temporary stopgap solution, while simultaneously increasing its elimination with diuretics. However, patients with moderate/severe renal dysfunction may need emergent haemodialysis. A subset of these patients will have chronic hyperkalaemia as a baseline that can be worsened with RAAS inhibitor administration. The objective of enduring treatment for chronic hyperkalaemia is to maintain stable serum potassium levels in the long term. If the baseline hyperkalaemia is too severe, and refractory to conservative measures (dietary modifications, diuretics, or oral potassium-binding agents), RAAS blockade may need to be stopped or reduced. Unfortunately, this leads to a loss or reduction of the benefits provided by these pharmaceuticals.
The rate of RAAS discontinuation in CKD patients is substantial. Conservative measures frequently fail because of patient intolerance to oral potassium-binding agents (resins). In one large study published by Olry de Labry Lima et al in 2021, ion-exchange resins were prescribed to 637 out of 1,499 patients receiving RAAS. Adherence to resin treatment was poor—36.8% in the first year and 17.5% by year three—and potassium levels remained elevated in most patients with severe hyperkalaemia. Two-year results from this study can be seen below.
 In ESKD patients, the potential for hyperkalaemia increases as the time between dialysis sessions increases beyond 48 hours, which suggests that interventions to prevent hyperkalaemia may be more necessary when time between dialysis sessions is greater than 48 hours. This risk occurs every week, typically over weekends, when patients are unmonitored. The rates for emergent/emergency haemodialysis have been shown to be as high as 17.6% for hyperkalaemia in a cohort of ESKD patients followed for two years. It has also been shown that the rate of emergent, first-time dialysis in worsening CKD patients can be as high as 18–19%. Unplanned dialysis sessions are associated with increased morbidity and mortality, which makes preemptive detection for unplanned dialysis important too.
In ESKD patients, the potential for hyperkalaemia increases as the time between dialysis sessions increases beyond 48 hours, which suggests that interventions to prevent hyperkalaemia may be more necessary when time between dialysis sessions is greater than 48 hours. This risk occurs every week, typically over weekends, when patients are unmonitored. The rates for emergent/emergency haemodialysis have been shown to be as high as 17.6% for hyperkalaemia in a cohort of ESKD patients followed for two years. It has also been shown that the rate of emergent, first-time dialysis in worsening CKD patients can be as high as 18–19%. Unplanned dialysis sessions are associated with increased morbidity and mortality, which makes preemptive detection for unplanned dialysis important too.
The problem of anaemia
Anaemia is also a very frequent complication of CKD, affecting the majority of patients with Stage 5 failure. The anaemia creates a deficit in the delivery of oxygen to all parts of the body. Initially, the body compensates for the reduced oxygen supply by increasing the heart rate but, over time, this can lead to cardiac hypertrophy. Deterioration of cardiac function in turn results in renal hypoperfusion that activates the sympathetic nervous system, as well as the renin angiotensin and aldosterone systems. Together, these further impair renal function. This becomes a vicious cycle known as cardiorenal anaemia syndrome (CRAS, Type IV). The syndrome can be initiated either from primary heart failure (Types I and II), primary renal failure (Types III and IV), or a combination of both (Type V). In the case of renal initiation by CKD, the predominant cause is erythropoietin deficiency, where the production of erythropoietin from the interstitial fibroblasts within the kidneys is not sufficient to meet the demand for new haemoglobin. The severity of anaemia is directly related to the degree of kidney dysfunction—the kidneys manufacture 90% of the erythropoietin produced by the body.

The most recent Kidney Disease: Improving Global Outcomes (KDIGO) guideline recommends regular assessment of haemoglobin levels in CKD patients, with increasing frequency as kidney function declines. The guidelines also recommend beginning a trial of iron therapy initially. The target range here is 10–12g/dl in CKD patients. And, as a general recommendation, the KDIGO guidelines support the starting of erythropoiesis-stimulating agent (ESA) therapy with haemoglobin concentrations <10g/dl (<100g/l) after assessment of all the risks associated with the therapy.
Anaemia in the CKD setting significantly increases the risk of morbidity and mortality in these patients. For coronary artery disease-related events, the ARIC study showed an increase in hazard ratio from 1.7 to 3.5 in the absence, versus the presence, of anaemia. The control of anaemia is clinically important and, if iron supplementation is not successful, then ESA therapy is warranted. However, the dosage range and high cost of ESA drugs must be optimised based on an accurate picture of haemoglobin levels, and the target level. Unnecessarily low or high ESA dosing levels are associated with poor outcomes—as shown in the CHOIR trial. The composite primary outcome (death, congestive heart failure, stroke and myocardial infarction) was significantly higher in patients assigned to the higher haemoglobin target value of 13.5g/dl vs 11.3g/dl.32 in this study. Establishing the correct baseline haemoglobin measurement in patients is complicated by cyclic variability, which can be affected by volume status, and the ability to remotely monitor haemoglobin levels in CKD patients would allow optimisation of the ESA therapy and may lead to improved patient outcomes.
Oxygen saturation, heart rate and auscultation
The kidney is particularly vulnerable to hypoxic events. Adequate oxygenation in patients with CKD may be impaired by a number of factors, including low haemoglobin and heart failure. Obstructive sleep apnoea (OSA) is also commonly found in patients with CKD (up to 80%) and there are currently hypotheses that the two are related. In a 2016 paper, Fahad Aziz and Kunal Chaudhary point out that OSA, CKD and hypertension are seen together as a common triad of pathologies. Therefore, OSA impacts the progression of CKD by inducing multiorgan system pathologies, such as:
- Cardiovascular disease effects—hypertension, arterial wall stiffness and endothelial dysfunction
- Respiratory effects—direct hypoxia, which creates oxidative stress and inflammation
- Central nervous system effects—sympathetic dysregulation and renin-angiotensin system (RAS) activation
Not surprisingly, cardiac arrhythmias are not uncommon during hypoxic episodes. These arrhythmias may range from benign bradycardias to atrial fibrillation, and fatal ventricular tachycardias. Gami et al report in the Journal of the American College of Cardiology that the magnitude of nocturnal hypoxaemia was an independent predictor of the onset of atrial fibrillation. The new onset of nocturnal desaturations or severe desaturations should prompt treatment to limit the adverse consequences in a CKD patient and, as such, the ability to remotely, non-invasively monitor these parameters is critical in this patient population.
Finally, haemodialysis is dependent on reliable access to the central circulation for repetitive dialysis sessions. A mature AVF offers the best opportunity for a durable and lasting solution. However, it is still susceptible to a number of potential complications that include stenosis, thrombosis, aneurysms, limb ischaemia, and infection.
Primary patency refers to the time until the first procedure or the occurrence of occlusion—whichever occurs first. Assisted primary patency refers to a vascular access that has been intervened upon prior to failing. Unfortunately, the literature indicates that up to 50% of AVFs never mature to the extent that they can support haemodialysis, although the ability to intervene early in vascular access dysfunction prior to its failure significantly increases the likelihood of long-term success. Secondary patency refers to the salvage of a thrombosed arteriovenous access. However, AVFs that have thrombosed have a tendency for early re-thrombosis and, of the usable AVFs, 25% will fail after two years. In general, patency of fistulas and grafts is similar, but grafts tend to require more interventions to maintain adequacy for haemodialysis.
The KDOQI guidelines recommend frequent assessment and monitoring of these access sites every month for signs of malfunction. A well-accepted aspect of the physical examination—as described by Koirala et al in 2016—includes auscultation of the audible characteristics of the access site. These characteristics should generally be of a low frequency, holosystolic, undulating pitch. Indications of a significant stenosis or impending access failure include an increase in the audible pitch during systole only, harsh amplitudes, or a very weak signal altogether. The absence of a palpable thrill is an additional sign of possible access flow concerns. However, unfortunately, it is often difficult for nephrologists to evaluate the fistula at the time of the patient’s dialysis.
Stenosis leading to thrombosis is the primary cause of AVF failure. This is typically observed at the venous outflow and inflow. Surveillance of fistula or graft patency is an ongoing necessity, and the ability to remotely monitor the audible characteristics of a vascular access would be important in optimising access patency and successful dialysis. In conclusion, patients with CKD and ESKD are complex, and require careful and ongoing monitoring of critical indicators including physiologic parameters, such as heart rate, SpO2, and biomarkers, such as haemoglobin and potassium levels. Those patients with a vascular access in place also benefit from a diligent surveillance system to enhance the long-term patency of their access.
References:
- Bikbov B, Purcell CA, Levey AS, et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 2020;395(10225):709-733. DOI: 10.1016/s0140-6736(20)30045-3.
- Komenda P, Tangri N, Klajncar E, et al. Patterns of emergency department utilization by patients on chronic dialysis: A population-based study. PLoS One 2018;13(4):e0195323. DOI: 10.1371/journal.pone.0195323.
- Wiebe N, Klarenbach SW, Allan GM, et al. Potentially preventable hospitalization as a complication of CKD: a cohort study. Am J Kidney Dis 2014;64(2):230-8. (In eng). DOI: 10.1053/j.ajkd.2014.03.012.
- Ronksley PE, Tonelli M, Manns BJ, et al. Emergency Department Use among Patients with CKD: A Population-Based Analysis. CJASN 2017;12(2):304-314. (In eng). DOI: 10.2215/CJN.06280616.
- Lovasik BP, Zhang R, Hockenberry JM, et al. Emergency Department Use and Hospital Admissions Among Patients With End-Stage Renal Disease in the United States. JAMA Intern Med 2016;176(10):1563-1565. (In eng). DOI: 10.1001/jamainternmed.2016.4975.
- Kumar S, Jeganathan J, Amruthesh. Timing of nephrology referral: influence on mortality and morbidity in chronic kidney disease. Nephrourol Mon 2012;4(3):578-81. (In eng). DOI: 10.5812/numonthly.2232.
- Dogan E, Erkoc R, Sayarlioglu H, et al. Effects of late referral to a nephrologist in patients with chronic renal failure. Nephrology (Carlton) 2005;10(5):516-9. (In eng). DOI: 10.1111/j.1440-1797.2005.00433.x.
- Kim DH, Kim M, Kim H, et al. Early referral to a nephrologist improved patient survival: prospective cohort study for end-stage renal disease in Korea. PLoS One 2013;8(1):e55323. (In eng). DOI: 10.1371/journal.pone.0055323.
- Chen Y-Y, Chen L, Huang J-W, et al. Effects of Early Frequent Nephrology Care on Emergency Department Visits among Patients with End-stage Renal Disease. Int J Environ Res Public Health 2019;16(7):1158. (In eng). DOI: 10.3390/ijerph16071158.
- Wang AY, Lai KN. The importance of residual renal function in dialysis patients. Kidney Int 2006;69(10):1726-32. (In eng). DOI: 10.1038/sj.ki.5000382.
- Marrón B, Remón C, Pérez-Fontán M, et al. Benefits of preserving residual renal function in peritoneal dialysis. Kidney Int Suppl 2008(108):S42-51. (In eng). DOI: 10.1038/sj.ki.5002600.
- Dhondup T, Qian Q. Electrolyte and Acid-Base Disorders in Chronic Kidney Disease and End-Stage Kidney Failure. Blood Purif 2017;43(1-3):179-188. DOI: 10.1159/000452725.
- Olry de Labry Lima A, Diaz Castro O, Romero-Requena JM, et al. Hyperkalaemia management and related costs in chronic kidney disease patients with comorbidities in Spain. Clin Kidney J 2021;14(11):2391-2400. DOI: 10.1093/ckj/sfab076.
- Ingelfinger JR. A new era for the treatment of hyperkalemia? NEJM 2015;372(3):275-7. (In eng). DOI: 10.1056/NEJMe1414112.
- Di Lullo L, Ronco C, Granata A, et al. Chronic Hyperkalemia in Cardiorenal Patients: Risk Factors, Diagnosis, and New Treatment Options. Cardiorenal Med 2019;9(1):8-21. DOI: 10.1159/000493395.
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. European Heart Journal 2021;42(36):3599-3726. DOI: 10.1093/eurheartj/ehab368.
- Group KDIGOKCW. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of CKD. Kidney Int 2013;3(1):1-150.
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017;136(6):e137-e161. (In eng). DOI: 10.1161/cir.0000000000000509.
- Ng KE. Updated Treatment Options in the Management of Hyperkalemia. US Pharm 2017;42(2):HS15-HS18.
- Liu X, Dai C. Advances in Understanding and Management of Residual Renal Function in Patients with Chronic Kidney Disease. Kidney Diseases 2016;2(4):187-196. DOI: 10.1159/000449029.
- Palmer BF. Managing hyperkalemia caused by inhibitors of the renin-angiotensin-aldosterone system. NEJM 2004;351(6):585-92. (In eng). DOI: 10.1056/NEJMra035279.
- Yusuf AA, Hu Y, Singh B, et al. Serum Potassium Levels and Mortality in Hemodialysis Patients: A Retrospective Cohort Study. Am J Nephrol 2016;44(3):179-86. DOI: 10.1159/000448341.
- Li WY, Wang YC, Hwang SJ, et al. Comparison of outcomes between emergent-start and planned-start peritoneal dialysis in incident ESRD patients: a prospective observational study. BMC Nephrol 2017;18(1):359. DOI: 10.1186/s12882-017-0764-6.
- Fages V, de Pinho NA, Hamroun A, et al. Urgent-start dialysis in patients referred early to a nephrologist—the CKD-REIN prospective cohort study. Nephrology Dialysis Transplantation 2021;Advance Article:1-1.
- Mendelssohn DC, Malmberg C, Hamandi B. An integrated review of “unplanned” dialysis initiation: reframing the terminology to “suboptimal” initiation. BMC Nephrology 2009;10(1):22. DOI: 10.1186/1471-2369-10-22.
- Babitt JL, Lin HY. Mechanisms of anemia in CKD. J Am Soc Nephrol 2012;23(10):1631-1634. (In eng). DOI: 10.1681/ASN.2011111078.
- McCullough PA. Anemia of cardiorenal syndrome. Kidney Int Suppl (2011) 2021;11(1):35-45. DOI: 10.1016/j.kisu.2020.12.001.
- Tsuruya K, Eriguchi M, Yamada S, et al. Cardiorenal Syndrome in End-Stage Kidney Disease. Blood Purif 2015;40(4):337-43. DOI: 10.1159/000441583.
- Nolan KA, Wenger RH. Source and microenvironmental regulation of erythropoietin in the kidney. Curr Opin Nephrol Hypertens 2018;27(4):277-282. (In eng). DOI: 10.1097/mnh.0000000000000420.
- KDIGO Anemia Work Group. KDIGO clinical practice guideline for anemia. 2012.
- Astor BC, Coresh J, Heiss G, et al. Kidney function and anemia as risk factors for coronary heart disease and mortality: the Atherosclerosis Risk in Communities (ARIC) Study. Am Heart J 2006;151(2):492-500. (In eng). DOI: 10.1016/j.ahj.2005.03.055.
- Singh AK, Szczech L, Tang KL, et al for the CHOIR Investigators*. Correction of Anemia with Epoetin Alfa in Chronic Kidney Disease. NEJM 2006;355(20).
- Bellizzi V, Minutolo R, Terracciano V, et al. Influence of the cyclic variation of hydration status on hemoglobin levels in hemodialysis patients. Am J Kidney Dis 2002;40(3):549-55. (In eng). DOI: 10.1053/ajkd.2002.34913.
- Somkearti P, Chattakul P, Khamsai S, et al. Predictors of chronic kidney disease in obstructive sleep apnea patients. Multidiscip Respir Med 2020;15(1):470-470. (In eng). DOI: 10.4081/mrm.2020.470.
- Aziz F, Chaudhary K. The Triad of Sleep Apnea, Hypertension, and Chronic Kidney Disease: A Spectrum of Common Pathology. Cardiorenal Med 2016;7(1):74-82. DOI: 10.1159/000450796.
- Lin C-H, Lurie RC, Lyons O. Sleep Apnea and Chronic Kidney Disease – A State of the Art Review. Chest 2019.
- Gami AS, Hodge DO, Herges RM, et al. Obstructive sleep apnea, obesity, and the risk of incident atrial fibrillation. J Am Coll Cardiol 2007;49(5):565-71. (In eng). DOI: 10.1016/j.jacc.2006.08.060.
- Zoccali C, Roumeliotis S, Mallamaci F. Sleep Apnea as a Cardiorenal Risk Factor in CKD and Renal Transplant Patients. Blood Purif 2021;50(4-5):642-648. DOI: 10.1159/000513424.
- Schinstock CA, Albright RC, Williams AW, et al. Outcomes of arteriovenous fistula creation after the Fistula First Initiative. CJASN 2011;6(8):1996-2002. (In eng). DOI: 10.2215/CJN.11251210.
- Voorzaat BM, Janmaat CJ, van der Bogt KEA, et al. Patency Outcomes of Arteriovenous Fistulas and Grafts for Hemodialysis Access: A Trade-Off between Nonmaturation and Long-Term Complications. Kidney360 2020;1(9):916-924. DOI: 10.34067/kid.0000462020.
- Lok CE, Huber TS, Lee T, et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am J Kidney Dis 2020;75(4 Suppl 2):S1-S164. DOI: 10.1053/j.ajkd.2019.12.001.
- Gilmore J. KDOQI clinical practice guidelines and clinical practice recommendations–2006 updates. Nephrol Nurs J 2006;33(5):487-8. (In eng).
- Koirala N, Anvari E, McLennan G. Monitoring and Surveillance of Hemodialysis Access. Semin Intervent Radiol 2016;33(1):25-30. DOI: 10.1055/s-0036-1572548.
- Malovrh M. Strategy for the Maximal Use of Native Arteriovenous Fistulae for Hemodialysis. The Scientific World JOURNAL 2006;6:808-815. DOI: 10.1100/tsw.2006.171.
- Rohatgi R, Ross MJ, Majoni SW. Telenephrology: current perspectives and future directions. Kidney Int 2017;92(6):1328-1333. (In eng). DOI: 10.1016/j.kint.2017.06.032.
- Li L, Perl J. Can Remote Patient Management Improve Outcomes in Peritoneal Dialysis? Contrib Nephrol 2019;197:113-123. DOI: 10.1159/000496306.
DISCLAIMER: Caution – investigational device. Limited by United States law to investigational use.









