
This advertorial is sponsored by Phraxis, Inc.
Dialysis access is an issue encountered by all patients who need to undergo haemodialysis. The main options currently available for dialysis access—including arteriovenous fistulas (AVFs), arteriovenous grafts (AVGs) and catheters—are each accompanied by challenges that can mean they are not necessarily the “right access” for every dialysis patient. In a recent United States Renal Data System (USRDS) estimate, of 550,000 “maintenance” haemodialysis patients, 355,000 patients were using AVFs, 105,000 catheters and 90,000 AVGs. Of these patients, AVfs were found to have a greater patency, but approximately 50% of AVFs in the USA failed to mature; AVGs had great maturation, but they didn’t have the longevity of AVFs; and catheters caused both inflammation and blood stream infection.

Since the introduction of the Kidney Disease Outcomes Quality Initiative (KDOQI) in 2019, the “new mantra”, as Phraxis chief executive officer (CEO) Alexander Yevzlin phrased it, has been “the right patient, in the right access, at the right time, for the right reasons”, rather than the previous “fistula-first” approach. With AVFs no longer viewed as being preferable to AVGs, Phraxis set out to provide a solution to the gap in the market that they felt needed to be filled, for the benefit of both patients and clinicians.
Speaking to Renal Interventions, John Ross (Medical University of South Carolina, Orangeburg, USA) summarised the issues with AVGs. “We’ve been doing things with grafts—the same thing—for over five decades. And the failure mode is development of stenosis in the graft-vein anastomosis. Every access has its own peculiar failure mode, be it a fistula, be it a graft. One of the reasons grafts don’t last so long is not necessarily in the conduit of the graft itself; it’s at the graft-vein anastomosis. Numerous things have been tried after a surgical anastomosis had been made—we’ve got balloons, we’ve got drug-coated balloons, we’ve got all kinds of other devices that have been tried—and really nothing has worked effectively at all.”
Commenting on the inspiration for EndoForceTM Endovascular Anastomotic Connector (EndoForce Connector), Yevzlin stated that “when I started thinking about [these failure modes], I recognised early on that the disease state, the frequent interventions that occur in grafts specifically, occur at the venous anastomosis. Ninety percent of them are at the venous anastomosis, and wouldn’t it be nice if we had some kind of solution?”
The solution

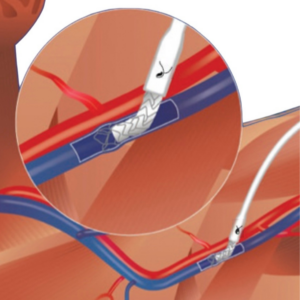
The solution is the EndoForce Connector, which is a patented implant for coaxial anastomosis of a vein to an AVG for haemodialysis, the EndoForce Connector is designed to provide an alternative, less traumatic endovascular venous anastomosis that can ameliorate the clinical challenges associated with a sutured anastomosis. It does this by having three distinct design elements: anchoring barbs that secure the device within the vein, a flexible segment comprised of expanded polytetrafluoroethylene (ePTFE)-covered nitinol within and at the vein junction, and a manually compressible ePTFE-covered nitinol segment that is fitted within the AVG that expands to fit against the wall of the AVG after insertion. The EndoForce Connector is designed for use with the physician’s choice of standard 6mm ePTFE AVG. In reducing the risk of venous anastomotic stenosis, the EndoForce Connector may potentially lead to extended graft patency, a reduction in repeat access surgeries, and a reduction in the need for catheter use.
The EndoForce procedure obviates the need remove the target vein out of its tissue bed, traumatise the vein with clamps, and sew the vein to ePTFE material. In addition, the end-to-end anastomosis of the EndoForce Connector, rather than the end-to-side of a traditional sutured AVG, allows for more laminar outflow, which may also reduce neointimal hyperplasia at the anastomosis. With the conventional end-to-side venous anastomosis, the vessel wall is subjected to turbulent, non-laminar flow and shear stress.
Positive, real-world results
To evaluate the safety and effectiveness of this novel device, a pivotal, prospective, multicentre, single-arm investigation trial was conducted. In this trial, 158 subjects with end-stage renal disease (ESRD) who had a planned AVG implant procedure for haemodialysis access and who met the study selection criteria, were enrolled at 10 locations in the USA. The primary endpoint was cumulative patency at six months, assessed by comparison to a performance goal of 75% (based on medical literature). Secondary endpoints included acute device success, primary unassisted patency at six months, time to first cannulation for haemodialysis, number and type of interventions required to maintain secondary patency, and number and type of serious adverse events through six months.
The results showed that the primary endpoint was met: AVGs implanted using the EndoForce Connector for the venous anastomosis had a cumulative patency at six months of 92% and an improvement when compared (although not directly) to traditional sutured AVGs (80%).3 They also showed a primary patency of 60% at six months and a procedural success rate of 100%, defined as AVG flow at the end of the procedure (determined by palpable graft thrill and/or audible bruit), without significant bleeding or need for emergent surgery.
Clinical investigators report that the EndoForce Connector may allow easier access to deep axillary veins.
Clinicians’ choice
Speaking to his experience using the EndoForce Connector during the investigational clinical study, Ari Kramer (Spartanburg Medical Center, Spartanburg, USA), explained: “I found the device to be intelligently designed, with an intuitive implantation technique which was easy to learn and employ, reduced my operating time, and facilitated both excellent and durable outcomes that outstripped our standard hand-sewn anastomoses. Overall, this is an outstanding and novel technology that should be welcomed in the AV access space.”
Ross, lead prinicpal investigator for the pivotal study, stated that “the EndoForce is giving us a completely different fluid dynamic, I think, at the graft vein anastomosis. The typical graft vein anastomosis is an end-to-side anastomosis, meaning that the blood itself is hitting, if you like, the opposite vein wall, causing an endothelial build-up, causing a stricture. With the EndoForce, what we’re doing is creating a functional end-to-end anastomosis. I believe it creates a laminal flow. Therefore, the failure mode is not going to be the stenosis nearly as much as we have seen with the traditional surgical anastomosis.”
Continuing, he added: “We want longevity out of our accesses. There are two things we need for access for the dialysis patient. Number one, you have to be able to get a cannula in it to get the blood out of the patient’s access over to a dialysis machine to be effectively dialysed. You need to have adequate flow to do that in the access, and we need to be able to cannulate the access. Then, what we would really want out of this is to get longevity out of the graft. We would like to see a long period of time so further interventions aren’t necessary [and] we want time without further interventions.”
The future of AV access
With the advent of KDOQI and the movement away from the “fistula-first” approach to AV access, it is important that new avenues for creating and improving accesses for haemodialysis emerge. With that in mind, Phraxis’ novel EndoForce Connector aims to transform the lives of ESRD patients by offering an alternative to the traditional sutured venous anastomosis.
The EndoForce Endovascular Anastomic Connector is an investigational device limited by US federal law to investigational use.
References
- Lok CE, Huber TS, Lee T, Shenoy S, et al. National Kidney Foundation. KDOQI clinical practice guideline for vascular access: 2019 Update. Am J Kidney Dis. 2020 Apr;75(4 Suppl 2):S1-S164.
- Burgess JS, Beaver JD, London M, et al. InterGraft Study Investigators. Prospective multicenter study of a novel endovascular venous anastomotic procedure and device for implantation of an arteriovenous graft for hemodialysis. J Vasc Access. 2023 Mar 9:11297298231159691.
- Halbert RJ, Nicholson G, Nordyke RJ, et al. Patency of ePTFE arteriovenous graft placement in hemodialysis patients: systematic literature review and meta-analysis. Kindey360. 2020, Dec 31; 1(12): 1437-1446. Published online 2020 Oct 15.









